| |
Rapid Resolution of Hepatitis C Virus-Associated Cryoglobulin Rash With Use of Direct-Acting Antivirals
|
| |
| |
Download the PDF here
Clinical Gastroenterology and Hepatology Nov 2015
Eric Chak,* Carl Schulze, and Bruce A. Runyon*
*Division of Digestive Diseases, Division of Nephrology, David Geffen School of Medicine at the
University of California Los Angeles, Los Angeles, California
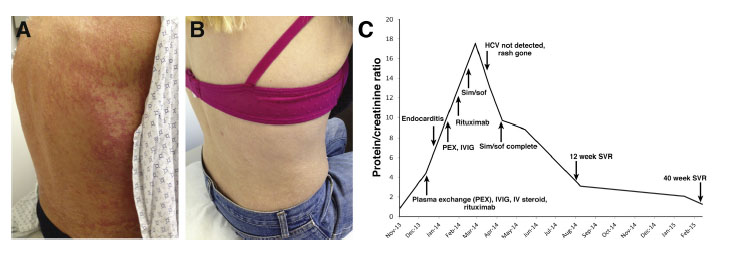
A 52-year-old woman with a 40-year history of a petechial, papular rash on her extremities and trunk (Figure A), chronic kidney disease stage III, and treatment-naive hepatitis C virus (HCV) genotype 1b with cirrhosis was admitted to the hospital for worsening renal failure, hypertensive urgency, and proteinuria. As a child she received multiple doses of immunoglobulin for tonsillitis in Hungary, likely contracting HCV through contaminated blood product or needles.
Her urine protein to creatinine ratio (Pr/Cr) was found to have increased sharply from 0.87 to 4.40 1 month before presentation and her blood pressure was 250/136. A prior liver biopsy showed chronic hepatitis with mild activity (grade 2 of 4) and periportal and focal bridging fibrosis (stage 3 of 4). An ultrasound of her abdomen showed an enlarged spleen (14.2 cm) and a complete blood count showed thrombocytopenia, both supporting the presence of cirrhosis with portal hypertension.
Serum cryoglobulins were detectable and acute kidney injury was present. A kidney biopsy was performed on the second hospital day, which was consistent with cryoglobulinemic glomerulonephritis complicated by moderate tubulointerstitial changes. Thus, plasma exchange, intravenous methylprednisolone pulse, intravenous immunoglobulin, and rituximab 375 mg/m2 were administered. Renal function was stabilized and she was discharged. A punch biopsy of her thigh confirmed vasculitis secondary to cryoglobulinemia.
She was re-admitted shortly thereafter for fever and was found to have endocarditis. She was treated with a 6-week course of intravenous antibiotics during which rituximab was held. For worsening proteinuria (Pr/Cr, 8.16) and rash, she was hospitalized for a third time for plasma exchange and an additional dose of intravenous immunoglobulin. Despite these interventions, there was minimal improvement in her rash and her proteinuria level continued to increase (peak Pr/Cr, 17.68). Three additional doses of rituximab 375 mg/m2 were given as an outpatient, but proteinuria remained persistent.
Simeprevir 150 mg and sofosbuvir 400 mg orally once daily were started for a 12-week course. The pretreatment HCV RNA level was 6,770,000 IU/mL. Other pertinent laboratory values included a total bilirubin level of 1.4 g/dL, aspartate aminotransferase level of 54 U/L, alanine aminotransferase level of 28 U/L, alkaline phosphatase level of 955 U/L, and albumin level of 3.1 g/dL. After 5 weeks of therapy, HCV RNA was undetectable and her rash was resolved clinically (Figure B). HCV RNA level measured at 12 weeks after treatment was undetectable and remained undetectable 40 weeks after finishing treatment. Proteinuria also has continued to improve because the Pr/Cr measured 10 months after treatment was 1.26. The patient's overall treatment course with respect to renal improvement is summarized in Figure C.
Despite achieving sustained virologic response, qualitative serum cryoglobulins remain positive and proteinuria, although vastly improved, remains present. She will unlikely achieve full renal recovery because moderate tubulointerstitial changes were seen on her kidney biopsy, indicating scarring. A large cohort study has suggested that persistent cryoglobulinemia in patients who achieve sustained virologic response occurs only 3% of the time.1 A possible explanation of this phenomenon is that occult HCV infection remains present in peripheral blood mononuclear cells, but remains undetectable in the serum and that persistent cryoglobulinemic syndrome is perpetuated through t(14;18) translocation-positive B-cell clones.2
|
|
| |
| |
|
|
|